What Causes Tuberous Breast Deformity?
Published by Reza Nassab
A tubular or tuberous breast deformity is a congenital (from birth) difference in how the breast develops, but it usually becomes noticeable during puberty when the breast starts to grow. Instead of expanding evenly into a rounded breast mound, growth is restricted at the breast base, so the breast can look:
-
Narrow at the base (the “footprint” on the chest wall is smaller than expected)
-
More conical or tubular
-
With a high breast fold (the crease under the breast sits higher)
-
With a puffy or enlarged areola, sometimes with breast tissue “pushing” into the areola (areolar herniation)
-
Underdeveloped lower breast (especially the lower inner and/or lower outer quadrants)
-
Asymmetrical (one side often worse than the other)
It’s important to say clearly: this is not your fault. It isn’t caused by bras, exercise, weight training, sex, pregnancy, or breastfeeding. It’s a developmental pattern that appears as your body matures.
What actually causes tuberous breasts?
The medical literature shows that there isn’t a single confirmed cause, and different patients may have slightly different underlying tissue factors.
Constricting “fibrous ring” restricts normal breast expansion
One of the most widely referenced explanations is that a tight ring/band of fibrous tissue (in the superficial fascia) forms around the breast, particularly affecting the lower part. When the breast tries to grow at puberty, it can’t expand outward and downward normally, so it is “redirected” forward—often towards the nipple–areola complex—creating the classic tubular shape and puffy areola.
Think of it like this:
-
A normal breast expands like a balloon inflating evenly.
-
A tubular breast is like a balloon with a tight tape band around its base—so it bulges where it can, rather than where it should.
What do studies show under the microscope?
Histological studies have found altered collagen patterns and differences in connective tissue arrangement in tuberous breasts compared with typical breast tissue. This supports the idea that connective tissue architecture plays a central role in the deformity.
Skin and breast “envelope” shortage contributes (especially in more severe cases)
Another important factor is relative skin deficiency, particularly in the lower breast. If the lower pole skin doesn’t expand adequately, the breast can look tight, high-riding, and underfilled below the nipple, even if there is some gland present. This concept is discussed in surgical literature describing the deformity as resulting from both constriction and skin shortage, with tissue herniation towards the areola in some patterns.
In practice, this is why some patients can look like they have:
-
A fairly “normal” upper breast
-
But a tight, underdeveloped lower breast
-
And a puffy areola that draws the eye
Is it genetic?
There are reports and clinical observations suggesting a genetic predisposition (for example, cases occurring in close relatives or twins), but the evidence is not strong enough to say tubular breasts are definitively inherited. Most reputable reviews describe genetics as a plausible contributor rather than a confirmed cause.
What we can say safely:
-
The condition is congenital
-
It likely involves connective tissue development
-
Genetics may influence connective tissue traits (like collagen behaviour), but that’s not the same as “one tubular breast gene”.
Does puberty “cause” tubular breasts?
Puberty doesn’t cause it, but puberty reveals it. Most authors describe tubular breasts as a congenital or developmental difference that becomes apparent when oestrogen-driven breast growth begins. That’s why many patients only realise something is different at ages 11–16, and why it can feel sudden and emotionally difficult.
What does not cause tubular breasts?
This matters, because patients are often (unfairly) hard on themselves.
Tubular breasts are not caused by:
-
Wearing the “wrong” bra
-
Not wearing a bra
-
Exercise or chest workouts
-
Poor posture
-
Sleeping position
-
Breastfeeding (though breastfeeding can reveal asymmetry in anyone)
-
A breast lump or cancer
Are tuberous breasts linked to problems with breastfeeding?
A subset of patients with tubular breasts also have reduced glandular tissue (hypoplasia/insufficient glandular tissue). That can increase the risk of low milk supply, but many patients breastfeed normally—especially in milder forms. If breastfeeding is important to you, this is something a specialist can discuss realistically, based on your anatomy.
Are there different “types” and does that affect the cause?
Clinically, yes—severity and pattern vary.
We often classify tuberous breasts by which parts of the lower breast are underdeveloped and how constricted the base is (several systems exist, and the details differ). In simple terms:
-
Mild: small lower inner deficiency, subtle constriction
-
Moderate: both lower quadrants affected, higher fold, more obvious shape change
-
Severe: major base constriction, significant underdevelopment, marked areolar herniation
Why this matters: different patterns may reflect different balances of constriction, skin shortage, and gland distribution—which is also why treatment planning is individual.
Common signs that suggest a tuberous breast deformity
Lots of patients are told they “just have small breasts”. The giveaway is that tubular breasts are usually about shape and base, not only size.
Look for:
-
Narrow breast base / breasts sit on a small footprint
-
Puffy, enlarged areola (sometimes “dome-like”)
-
Breast tissue seems to “point” forward rather than rounding out
-
Higher breast crease than expected
-
Empty-looking lower breast
-
Noticeable asymmetry (shape and/or crease height)
If you recognise yourself in this, a proper assessment is worthwhile—because standard augmentation alone can sometimes exaggerate the areola puffiness if the constriction isn’t addressed.
Why it can affect confidence
Even though tubular breasts aren’t dangerous, the psychological impact can be significant—especially because it commonly appears at a sensitive life stage. Many patients describe:
-
Avoiding bras/swimwear
-
Anxiety around intimacy
-
Feeling “abnormal” or “broken”
-
Frustration that friends’ bodies developed differently
These reactions are common and understandable. The aim of consultation isn’t to pressure surgery—it’s to give you clarity, options, and a plan that matches your goals. A recent article has been published in the Aesthetic Surgery Journal which highlights some of the psychological effects of tuberous breast deformity and breast surgery by Mr Nassab.
What to do if you think you have tubular breasts
Get a specialist assessment
A consultation should include:
-
Examination of base width, fold position, areola features, tissue distribution
-
Assessment of asymmetry
-
Discussion of your goals (natural vs augmented, subtle vs significant change)
Decide whether you want treatment
Some patients choose no treatment. Others choose correction because clothing fit, confidence, or asymmetry bothers them.
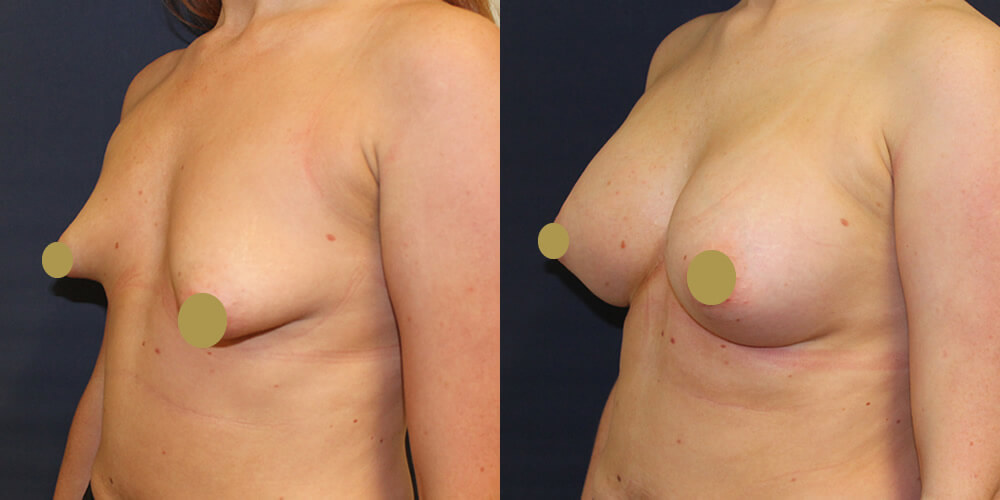
Surgical options
Surgical approaches vary (and can include scoring/releasing tight tissues, reshaping breast tissue, lift around the areola, implants and/or fat transfer, sometimes staged expansion in selected cases). The right plan depends on your anatomy and your preferences. Breast augmentation can provide volume to the breasts which can improve the shape to a more round rather than conical shape.
FAQs
Are tubular breasts rare?
They’re described as uncommon, but many experts believe they’re under-recognised, especially milder forms.
Can tuberous breasts happen on one side only?
Yes. Asymmetry is common, and one breast may be clearly more constricted than the other.
Will pregnancy fix tubular breasts?
Pregnancy can increase volume in many breasts, but it doesn’t reliably correct the underlying constriction, and asymmetry may persist or become more noticeable.
Is this a medical problem or cosmetic?
It isn’t dangerous, but it can affect wellbeing, body image, and sometimes breastfeeding capacity in a subset. It sits in the space where physical anatomy and mental wellbeing overlap.
Can a normal breast augmentation correct it?
Sometimes it helps volume, but if the constriction and areola herniation aren’t addressed, implants alone can give an “operated” look or worsen areola prominence. That’s why tuberous correction is treated as a specialist type of breast surgery. We can sometimes release the lower pole of the breast to allow expansion but sometimes areolar surgery may also be required which has additional scarring.
Medical references
-
Lozito A, et al. Review of Tuberous Breast Deformity. (2022).
-
Klinger M, et al. Tuberous breast: morphological and histological study. (2011).
-
van Durme J, et al. The Different Surgical Strategies for Treating Tuberous Breast… (2024).
-
Rees TD, Aston SJ. The tuberous breast. (1976).
-
Pacifico MD, et al. The tuberous breast revisited. (2007).